
Acute tonsilitis & chronic tonsilitis
Acute tonsillitis & chronic tonsillitis
We have described in article :
Classification of tonsillitis
Management of acute tonsillitis
Management of chronic tonsillitis
Malignant tumours of tonsil
Anatomy of the tonsil
Classification of tonsillitis :
1) Acute tonsillitis :
- Acute catarrhal or superficial tonsillitis.
- Acute follicular tonsillitis.
- Acute parenchymatous tonsillitis.
- Acute membranous tonsillitis.
Chronic tonsillitis :
- Chronic follicular tonsillitis.
- Chronic parenchymatous tonsillitis.
- Chronic fibroid tonsillitis.
Aetiology of tonsillitis :
Bacterial causes :
- Streptococcus beta haemolyticus
- Staphylococcus
- Haemophilus influenzae
- Pneumococcus.
Viral causes :
- Influenza virus
- Para influenza virus
- Adeno virus
- Rhino virus.
Acute tonsillitis:
Definition of acute tonsillitis : It is an acute inflammation of palatine tonsil.
Incidence:
- Acute tonsillitis often affects school-going children, but also affects adults.
- It is rare in infants and in persons who are above 50 years of age.
Symptoms of acute tonsillitis :
- Sore throat-uneasiness or foreign body sensation during swallowing
- Difficulty on swallowing
- Fever
- Earache
- Constitutional symptoms:
- Headache
- General body aches.
- Malaise
- Constipation.
- There may be abdominal pain.
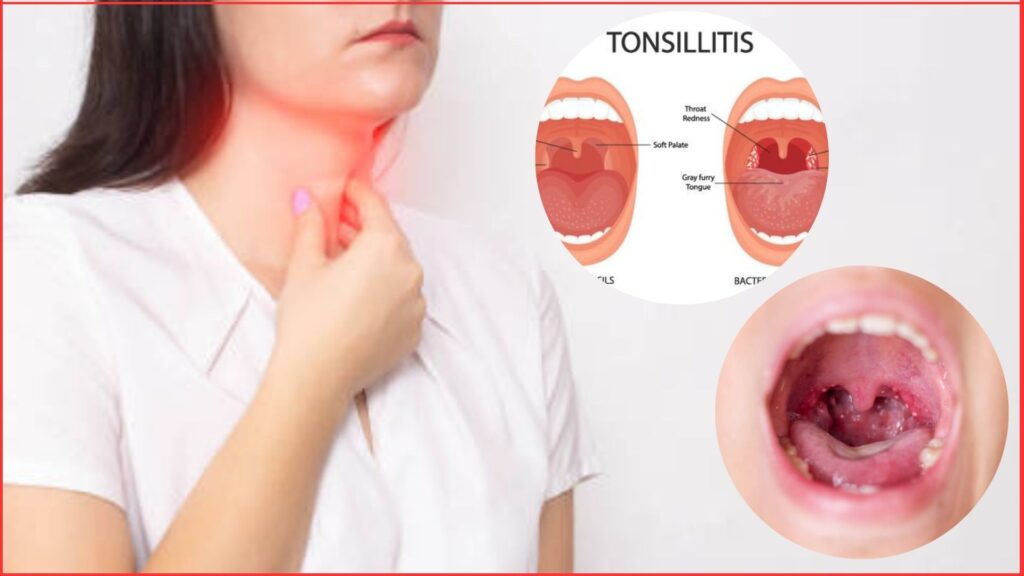
Signs of acute tonsillitis :
- Often the breath is foetid and tongue is coasted.
- Hypersemia of pillars, soft palate and uvula
- Tonsils are red and swollen with yellowish spots of purulent material presenting at the opening of crypts (acute follicular tonsillitis) or there may be a whitish membrane on the medial surface of tonsil which can be easily wiped away with a swab (acute membranous tonsillitis).
- The tonsils may be enlarged and congested so much so that they almost meet in the midline along with some oedema of the uvula and soft palate (acute parenchymatous tonsillitis).
- Temperature-102°F to 104°F.
- Enlarged, tender, jugulo-digastric lymph node or tonsillar lymph node.
Investigations of acute tonsillitis :
- Throat swab for culture & sensitivity.
- Blood for TC & DC of WBC, ESR.
Treatment acute tonsillitis :
General treatment :
- Bed rest
- Soft diet.
- More fluid intake.
- Warm saline gurgling
- Vitamin C is sometimes helpful.
- Tepid sponging.
Specific treatment :
Systemic antibiotics-Penicillin is the drug of choice.
- Oral Penicillin-V 250 mg every 6 hourly for 5-7 days.
- Amoxicillin 50 mg/kg body weight every 8 hourly for 5-7 days.
Analgesics to relieve pain & antipyretics.
Complications of acute tonsillitis :
- Chronic tonsillitis with recurrent acute attacks.
- Peritonsillar abscess.
- Parapharyngeal & retropharyngeal abscess.
- Cervical abscess.
- Acute otitis media.
- Rheumatic fever.
- Acute glomerulonephritis.
- Subacute bacterial endocarditis.
Differential diagnosis of white patch on the tonsillitis:
- Membranous tonsillitis.
- Diphtheria.
- Vincent’s angina.
- Infectious mononucleosis.
- Agranulocytosis.
- Leukaemia.
- Aphthous ulcers.
- Malignancy tonsil.
- Traumatic ulcer.
- Candidal infection of tonsil.
Chronic Tonsillitis :
Definition of chronic tonsillitis : It is the chronic inflammation of palatine tonsils where inflammation & repair goes side by side.
Incidence :
- Chronic parenchymatous tonsillitis: Seen in children & adolescents.
- Chronic follicular & fibrotic tonsillitis: Adults are usually affected.
3 important causes of unilateral tonsillar enlargement:
- Tonsillitis
- Peritonsillar abscess
- Tonsillar neoplasm
Symptoms of Chronic tonsillitis :
- Recurrent attacks of sore throat or acute tonsillitis.
- Chronic irritation in throat with cough.
- Bad taste in mouth and foul breath (halitosis) due to pus in crypts.
- Thick speech
- Difficulty in swallowing.
- Choking spells at night.
Signs of chronic tonsillitis :
- Tonsils may show varying degree of enlargement.
- There may be yellowish beads of pus on the medial surface of tonsil.
- Tonsils are small but pressure on the anterior pillar expresses frank pus (inspissated pus) or cheesy material.
- Flushing of anterior pillars.
- Non-tender bilateral palpable enlarged jugulo-digastric lymph node.
Investigations of chronic tonsillitis :
- Throat swab for culture & sensitivity.
- Blood for TC & DC of WBC.
Treatment of chronic tonsillitis :
- Conservative treatment : Attention to general health, diet, treatment of coexistent infection of teeth, nose and sinuses.
- Surgical treatment : Tonsillectomy under G/A.
MALIGNANT TUMOURS OF THE TONSIL / CARCINOMA TONSIL
Two malignancies of the palatine tonsil;
- Squamous cell carcinoma.
- Adenocarcinoma.
- Lymphoma.
- Sarcoma.
Malignant tumours of the tonsil:
Introduction of the malignant tumours : Squamous cell carcinoma is the most common & presents as an ulcerated lesion with necrotic base. Adenocarcinoma, lymphoma, sarcoma etc. may also occur. Lymphomas may present a unilateral tonsillar enlargement with or without ulceration & may simulate indolent peritonsillar abscess.
Clinical features of malignant tumour :
- Average age: 50-60 years.
- Sore throat.
- Difficulty in swallowing
- Pain in the ear.
- Lump in the neck
- Speech is altered as the growth involves pillars & tongue.
- Later, bleeding from the mouth, felor oris & trismus may occur.
- On examination :
- In early stage there is localized ulcerative lesion on the tonsil with induration.
- The tonsil is mobile in early stage, but gets fixed as the growth spreads to the pillars, tonsillo-lingual sulcus & the tongue.
- Metastasis in the upper deep cervical or jugulodigastric node is common.
Investigations :
- In early suspected ulcer on the tonsil & in unilateral tonsillar enlargement, whole tonsalis removed (tonsillectomy biopsy) & sent for histopathological examination.
- In advanced stage punch biopsy & histopathology is performed.
Treatment of tumours of the tonsil :
Radiotherapy : Early & radiosensitive tumours are treated by radiotherapy along with irridation of cervical nodes.
Surgery :
- Excision of the tonsil can be done for early superficial lesion.
- Larger lesion & those which invade bone require wide surgical excision with hemimandibulectomy & neck dissection (Commando operation).
Combination therapy :
- Surgery may be combined with pre or post-operative radiation.
- Chemotherapy may be given as an adjunct to surgery or radiation.
Anatomy of the Tonsil
The palatine tonsils : Tonsils are bilateral ovoid mass of lymphoid tissue on the lateral wall of the pharynx occupying the interval between the anterior & posterior pillar of fauces.
Anatomy of the tonsil :
It has
Two surfaces :
- Medial surface : Lined by the nonkeratinizing stratified squamous epithelium. Openings of 12- 15 crypts can be seen on the medial surface of the tonsil Largest one is called Crypta Magna or intratonsillar cleft.
- Lateral surface : Lateral surface of the tonsil presents a well-defined fibrous capsule.
Two poles :
- Upper pole : Related to the soft palate.
- Lower pole : Related to the base of the tongue. The tonsil is separated from the tongue by a sulcus called tonsillolingual sulcus which may be the seat of carcinoma.
Two borders :
- Anterior border : Related to the palatoglossal arch with its muscle.
- Posterior border : Related to the palatopharyngeal arch with its muscle.
Two folds :
- Plica semilunaris : A triangular vestigial fold of mucous membrane covering the anteroinferion part of the tonsil.
- Plica triangularis : A similar semilunar fold that may cross the upper part of the tonsil.
Blood supply of the tonsil :
Artery supply :
1). Main source : Tonsillar branch of facial artery
2) Additional sources :
- Ascending palatine branch of facial artery.
- Dorsal lingual branches of the lingual artery.
- Ascending pharyngeal branch of the external carotid artery.
- The greater palatine branch of the maxillary artery.
Venous drainage : Veins from the tonsils drain into paratonsillar vein which joins the common facial vein & pharyngeal venous plexus.
Lymphatic drainage :
- Send efferent vessels to the upper deep cervical group.
- Most of them end in the jugulodigastric lymph node.
Nerve supply : By-
- Lesser palatine branches of sphenopalatine ganglion (CNV).
- Glossopharyngeal nerve.
Formation of tonsillar bed :
- The bed of tonsil is formed from within outwards by
- Pharyngobasilar fascia.
- Superior constrictor & palatopharyngeus muscles.
- Buccopharyngeal fascia
- Lower part of the styloglossus.
- Glossopharyngeal nerve.
Boundaries of tonsillar sings or fossa/peritonsillar space :
In front : Palatoglossal arch containing the corresponding muscle
Behind : Palatopharyngeal arch containing the muscle of the same name.
Apex : By the soft palate where both arches meet.
Base : By the dorsal surface of the posterior one-third of the tongue.
Functions of tonsil :
They act as sentinels to guard against foreign intruders like viruses, bacteria and other antigens coming into contact through inhalation and ingestion. There are two mechanisms.
- Providing local immunity.
- Providing a surveillance mechanism so that entire body is prepared for defence.
you are really a good webmaster. The website loading speed is amazing. It seems that you are doing any unique trick. Furthermore, The contents are masterpiece. you’ve done a magnificent job on this topic!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good. https://accounts.binance.info/register?ref=P9L9FQKY